Can Adults Develop Scoliosis? Daily Recommendations for Maintaining Spinal Health
Contrary to popular belief, scoliosis (curvature of the spine) is not a condition exclusive to children. Yes, scoliosis can also occur in adults, and its prevalence may even increase with age. However, the process in adults differs from that in children.
In this article, we will focus on what you need to change in your daily life to maintain your spinal health in adulthood and build resistance to potential curvatures.
What Causes Scoliosis in Adults?
There are generally two factors underlying the spinal problems we encounter in adulthood:
- The Legacy of Childhood: A very slight curvature that goes unnoticed during adolescence may become slightly more pronounced over the years due to the effects of gravity.
- Ageing Effect: Just as our faces wrinkle and our hair turns grey, our spine also ages. The loss of fluid in the discs between the vertebrae and the wear and tear of the joints can disrupt the balance of the spine, leading to "secondary" curvatures.
So, what can we do to slow down the progression of scoliosis in adults or keep our spine strong against this wear and tear?
5 Golden Tips for a Spine-Friendly Life
Before resorting to medical interventions, making small changes to your lifestyle is the most effective remedy for relieving the strain on your spine.
1. Strengthen your "natural corset"
Your spine is not a pillar that carries your body on its own; it is surrounded by muscles. The stronger your abdominal and back muscles are, the less load is placed on your spine (bones). We call this the body's "natural corset".
- Suggestion: Do exercises that work the muscles around the spine at least 2-3 days a week, ensuring they are non-impact (do not require jumping). Swimming and Pilates are among the best spine-friendly sports.
2. Challenge Inactivity
The modern-day affliction of "inactivity" is the greatest enemy of spinal health. Sitting in the same position for long periods increases pressure on the discs.
- Suggestion: If you work at a desk, be sure to stand up every 45 minutes, walk for 2 minutes or do some simple stretching exercises. Your spine needs movement to stay healthy.
3. Be Mindful of Technology Use: Scoliosis in Adults
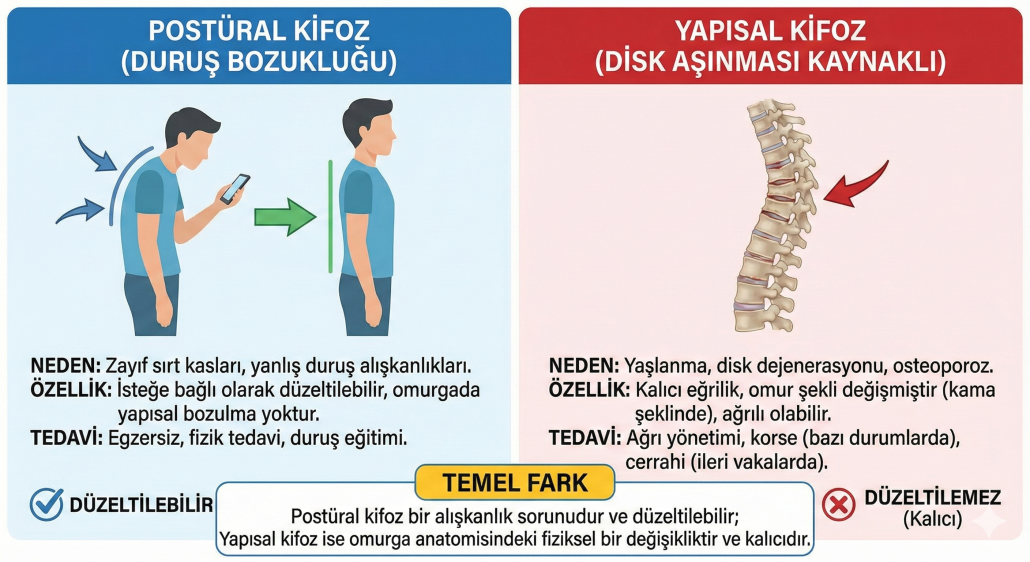
Nowadays, we constantly bend our heads forward to look at our smartphones. Every centimetre the head bends forward increases the load on the neck and spine. Over time, this can lead to poor posture and hunching of the back (kyphosis).
- Suggestion: Try to hold the phone at eye level, not at chest or stomach level. The top edge of your computer screen should be at eye level.
4. Weight Control is Important
Every extra pound on your body means extra weight for your spine to carry. Fat around your belly especially shifts your centre of gravity forward, putting pressure on the curve in your lower back (lordosis) and throwing your spine off balance.
- Suggestion: Maintaining your ideal weight is vital not only for your heart health but also for your spinal mechanics.
5. Support Bone Quality
With age, a decrease in bone density (osteoporosis) can lead to compression fractures in the vertebrae and associated curvature. The harder and stronger your bones are, the straighter your spine will be.
- Suggestion: Eat a balanced diet. Have your calcium and vitamin D levels monitored by your doctor. It is also a scientific fact that smoking impairs the nutrition of the discs, accelerating wear and tear; stay away from cigarettes for the sake of your spine.
When Should You Consult a Specialist?
Back pain is something everyone experiences from time to time. However, if the following situations apply, it is advisable to see a specialist rather than dismissing it as "old age" or "I caught a chill":
- If the pain does not go away with rest and wakes you up at night,
- If you notice a visible asymmetry (shift) in your back or waist,
- If you feel the need to lean forward while walking,
- If you notice a change in the fit of the clothes you wear.
Remember: the better you look after your spine, the longer and straighter it will carry you.
Frequently Asked Questions (FAQ)
Can postural problems in adults be corrected with exercise? If the problem is not a permanent curvature (scoliosis) but rather a postural problem caused by muscle weakness, then yes, significant improvements can be achieved with regular exercise and posture awareness.
Does mattress choice affect scoliosis in adults? Mattress choice does not cause scoliosis or improve an existing condition. However, to maintain spinal health and manage pain, mattresses of medium firmness that fill body contours should be preferred – neither too firm nor so soft that you sink into them.
Should I wear a brace to prevent scoliosis in adults? Should I wear a brace for prevention? It is not advisable to use ready-made braces available on the market without a doctor's recommendation, simply to avoid back pain or to stand up straight. Wearing these braces for extended periods can weaken your muscles, leading to muscle atrophy and exacerbating the problem.